Introduction
Cancer is the leading cause of death worldwide, and its incidence is still rising. Over the past half century, there has been significant progress in basic and clinical research on cancer, with a decline in the incidence and mortality of certain cancers. This is largely due to primary prevention (e.g., smoking cessation) and early cancer screening, rather than the effectiveness of any particular drug.[1] The current treatments including radiotherapy, chemotherapy, fine-needle puncture and surgery can be a double-edged sword, because their use can increase circulating tumor cells, and promote cancer progression and distant metastasis.[2],[3],[4],[5],[6] Precision treatment strategies based on molecular detection have not shown benefit in most cancer patients, with the development of precision drugs available for only 3–13% of patients.[7],[8] Studies have shown that targeted therapy induces high proteome secretion, leading to cancer metastasis.[9] Thus, alternative cancer treatments are required to avoid these challenges.
Molecular hydrogen biology and hydrogen therapy are new and rapidly developing areas of research.[10]-[12] Hydrogen has been shown to exert antioxidant and anti-inflammatory effects, and since the occurrence and progression of cancer are closely related to peroxidation and inflammation, hydrogen may play a role in the control of cancer. Using the “real world evidence” method,[13],[14],[15] we conducted a retrospective and prospective follow-up study on advanced cancer patients recovering from hydrogen therapy.
Subjects and Methods
Subjects
We analyzed two sets of patients: (1) Retrospective investigation of patients (n = 14) treated with hydrogen inhalation at home from March 2014 to April 2018, mainly through home visits and hospital medical records. (2) Prospective study of 68 patients enrolled after May 2018. Hydrogen inhalation was carried out mainly in the Guangdong Xukecheng Health Care Studio, China. Specialized doctors provided care and guidance to the volunteers, reviewed relevant materials as required, and carried out “prospective” observational studies. The study protocol received ethical approval from the Ethics Committee of Fuda Cancer Hospital of Jinan University on December 7, 2018 (approval number: Fuda20181207) and conformed to the specifications of the World Medical Association’s Declaration of Helsinki. Written informed consent was obtained from each participant. This study followed the STrengthening the Reporting of OBservational studies in Epidemiology (STROBE) Statement.
All patients who met the following inclusion criteria were included: (1) advanced cancer patient according to definite pathological and imaging diagnosis; (2) the patient failed to respond to conventional treatments, could not receive conventional treatment due to systemic conditions and diseases, or rejected the conventional treatments; (3) the patient had other symptoms, such as poor appetite, fatigue, insomnia and pain; (4) the patient with existing tumors or/or abnormal tumor markers; (5) aged 20–80 years, without obvious cardiac, cerebral, pulmonary and renal failure and mental abnormalities, able to describe symptoms.
Hydrogen inhalation method
Hydrogen was produced by a hydrogen-oxygen nebulizer (license No: AMS-H-01, Shanghai Asclepius Meditec Co., Ltd., Shanghai, China). The patient remained seated or recumbent, inhaled a mixture of hydrogen (66.7%) and oxygen (33.3%) with spontaneous breathing in a nasal tube or mask and a gas flow rate of 3000 mL/min. The hydrogen inhalation should be continued for > 3 hours per day for at least 3 consecutive months.
Imaging evaluation
Responses were evaluated according to the RECIST (Response Evaluation Criteria in Solid Tumors) criteria on the basis of changes in tumor size detected by computed tomography or magnetic resonance imaging as follows[16]: complete response (CR), all the target lesions disappeared, no new lesions appeared, and the tumor markers were normal for at least 4 weeks; partial response (PR), reduction in the maximum diameter of the target lesion by 30% for at least 4 weeks; stable disease (SD), the sum of the maximum diameter of the target lesion did not decrease by PR or increase by progressive disease; progressive disease, the maximum diameter of the target lesion increased by at least 20%, or new lesions appeared. The disease control rate (DCR) was calculated as CR + PR + SD as a proportion of the total number of patients treated.
Quality-of-life score
Patient quality-of-life was evaluated using the Quality of Life Questionnaire Core 30 (QLQ-C30) scale of the European Organization for Research and Treatment of Cancer.[17] The QLQ-C30 scale has a total of 30 items including 5 functional subscales (physical function, role function, cognitive function, emotional function and social function) and 3 symptom subscales (fatigue, pain, nausea/vomiting), 6 individual measures and 1 overall quality-of-life scale. Evaluation was conducted every other week before and after hydrogen inhalation. The evaluation was performed by a clinician who was blinded to the disease condition.
Physical condition score
The physical condition of patients was evaluated before and after treatment using the five-point Zubrod-ECOG-WHO score system of the United States’ Eastern Cooperative Oncology Group (ECOG). Physical condition was classified as follows: improvement, score decrease of 1 point or more; deterioration, score increase of 1 point or more; stability, no change in score.
Detection of tumor markers
Serum tumor markers were measured using an automatic electrochemiluminescence system (e 411; Roche, Basel, Switzerland) for quantitative determination of markers including alpha fetal protein, carcinoembryonic antigen (No. 11731629, Roche), carbohydrate antigen (CA)19-9 (No. 11776193, Roche), CA125 (No. 11776223, Roche), and CA153 (No. 03045838, Roche).[18] The selection of these markers was based on abnormal indicators reported in the medical records, with each patient having a range of elevated markers (0, 1 or multiple) at the time of diagnosis.
Statistical analysis
Paired t-tests were used to analyze differences in quality-of-life scores between groups, and chi-squared tests were used to analyze differences in physical fitness, tumor markers and imaging evaluation between groups. Significant differences were indicated by P < 0.05. All analyses were conducted using GraphPad software (GraphPad Software, San Diego, CA, USA).
Results
Clinical data of 82 advanced cancer patients treated with hydrogen inhalation rehabilitation
A total of 82 patients were followed up (14 at home and 68 patients in our clinic). The clinicopathological data of patients who received hydrogen inhalation therapy are shown in [Table 1].
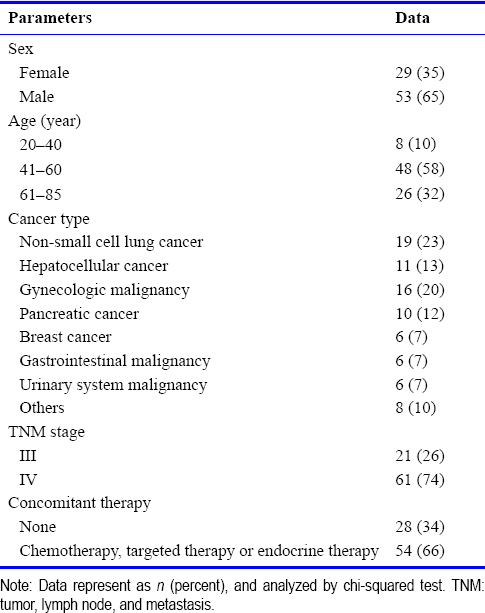
Table 1: Clinicopathological data of advanced cancer patients who received hydrogen inhalation therapy
Follow-up time and survival of 82 advanced cancer patients treated with hydrogen inhalation rehabilitation
All patients were followed up for 3–46 months, with a median time of 6 months. The follow-up continued for 3–6 months in 45 cases (55%), for 7–12 months in 33 cases (40%), and only in 1 case each for 13, 14, 26 and 46 months. Twelve patients died (all in stage IV), with four cases of pancreatic cancer (all tumor progression), two cases of liver cancer (liver failure and infection for one case each), one case of lung cancer (programmed cell death protein-1 (PD-1) antibody-associated pneumonia), three cases of gynecologic malignancy (one case each of intestinal obstruction, abdominal infection, and tumor progression), one case of gastrointestinal malignancy (massive upper gastrointestinal bleeding), and one other case (infection).
Quality-of-life
Thirty patients were prospectively evaluated by the QLQ-C30 score. After 2 weeks of hydrogen inhalation, patients reported a reduction in dyspnea and an increase in appetite, as well as significant improvements in their physical, role, and emotional functions, with reduced fatigue, nausea, vomiting, and insomnia. After 4 weeks of treatment, cognitive function, pain, appetite, constipation and diarrhea were all significantly improved [Table 2].
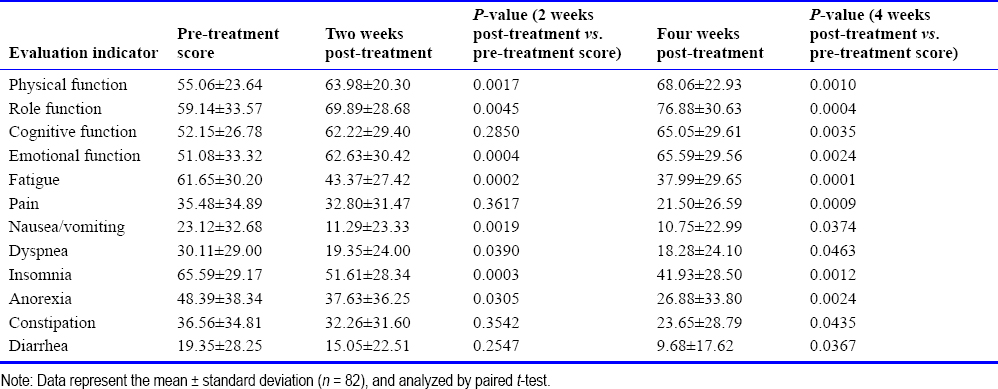
Table 2: Quality-of-life scores of advanced cancer patients who received hydrogen inhalation therapy
Physical fitness evaluation
The physical fitness of patients was evaluated using the Zubrod-ECOG-WHO score system. After 3 months of hydrogen inhalation therapy, 42% of the patients showed improvement in physical condition, 34% showed stability, and 24% showed deterioration. The improvement rate in patients treated with hydrogen inhalation alone was 32%, and that of patients who received hydrogen inhalation therapy combined with other treatments was 44%; and there was no significant difference between the two groups (P = 0.295). Compared with before treatment, the improvement rate of stage III patients was 57%, and that of stage IV patients was 36%, with no significant difference between the groups (P = 0.572). There was variation in the improvements in physical fitness among patients with different tumor types. The greatest improvement in physical fitness was observed in lung cancer patients (68%), while pancreatic cancer patients (0%) and patients with gynecological tumors (12%) showed the least improvement. The improvement of patients with lung cancer was significantly greater that of patients with gynecological and pancreatic cancers [Table 3].
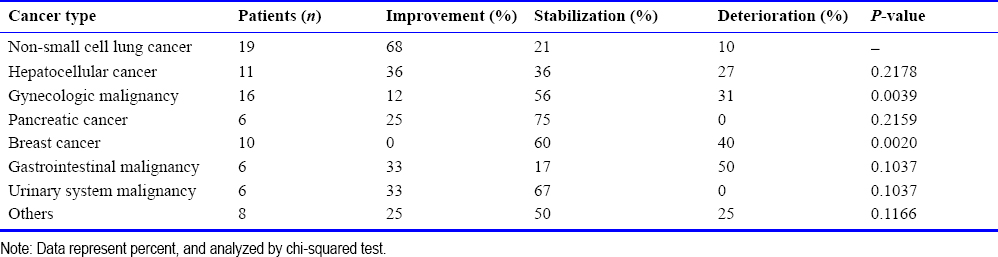
Table 3: Physical status of advanced cancer patients with different cancer types
Changes in tumor markers of 82 advanced cancer patients treated with hydrogen inhalation rehabilitation
Before hydrogen treatment, a total of 58 patients had elevated tumor markers. Three months after hydrogen treatment, tumor markers were decreased in 36% of patients, 16% showed no changes and 48% showed increase. Typical cases with decreased tumor markers are shown in [Figure 1]. The initial decline in tumor markers occurred over the period of 13–45 days (median 23 days) after treatment. Compared with the expression levels before treatment, the decrease in tumor marker expression in the patients who received hydrogen inhalation therapy alone and those who received combined treatments was 22% and 42%, respectively, with no significant difference between the two groups of patients (P = 0.3131). No elevation of tumor markers was observed after hydrogen inhalation therapy in patients with normal tumor markers before treatment. Fifty-eight patients with elevated biomarkers were analyzed according to their different tumor types. After 3 months of hydrogen inhalation therapy, the greatest decrease in tumor markers was observed in patients with lung cancer (75%), while no decrease was observed in patients with pancreatic and liver cancers [Table 4]. There were significant differences in the changes in tumor markers post-treatment between patients with lung cancer and those with gynecologic, liver cancer and pancreatic cancer.
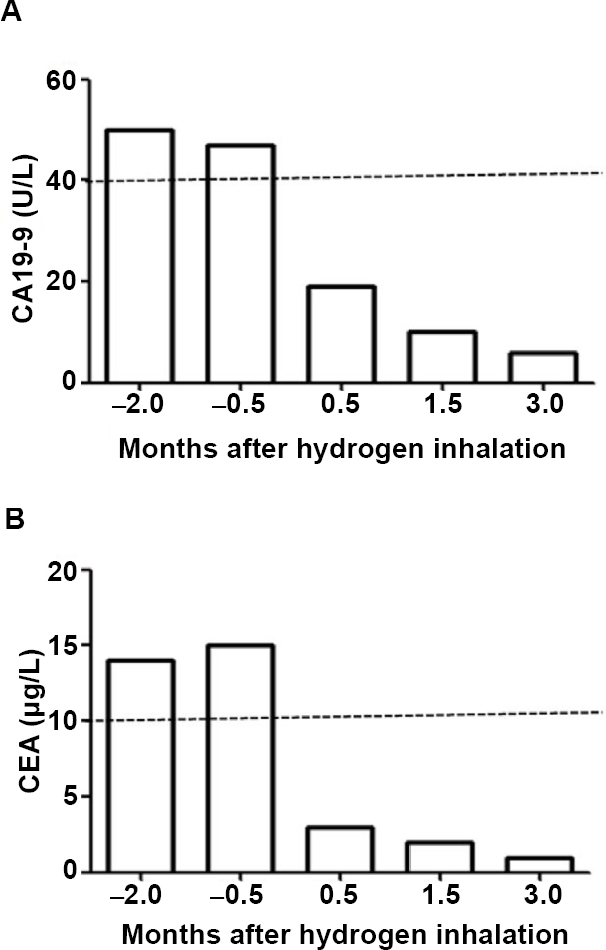
Figure 1: The tumor markers were decreased in the typical advanced cancer cases treated with hydrogen inhalation rehabilitation.
Note: (A, B) Miss Y, 28 years old. The uterus and attachments were removed because the left ovarian cancer in December 2017. After 3 months, the tumor marker examination was elevated twice, and there were no symptoms on computed tomography, ultrasound, and endoscopy. Hydrogen inhalation began on May 9, 2018, 3–4 hours daily. After 2 weeks, the tumor markers CA19-9 (A) and carcinoembryonic antigen (CEA) (B) were reviewed and completely reduced to normal (dotted lines in the figure). Until the beginning of 2019, there was no recurrence.Click here to view
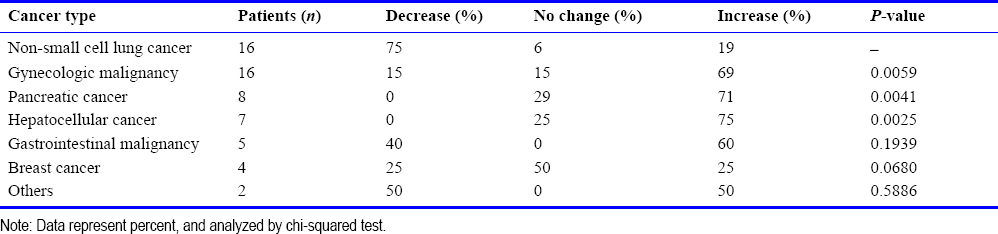
Table 4: Changes in tumor markers in advanced cancer patients with different tumor types
Tumor response of 82 advanced cancer patients treated with hydrogen inhalation rehabilitation
Of the 82 patients who participated in the study, 80 had tumors before enrollment, and the other two patients only had elevated tumor markers. Among the 80 patients with tumors, one (1%) showed CR, 15 (19%) showed PR, 30 (38%) showed SD, and 34 (42%) showed progressive disease after 3 months of hydrogen inhalation treatment, with a DCR of 57.5%. The typical case of tumor reduction is shown in [Figure 2]. CR and PR occurred within 21–80 days, with a median time of 55 days. The DCR in the patients who received hydrogen inhalation therapy only was 54%, and 59% in the patients who received hydrogen inhalation therapy combined with other treatments, with no significant difference in the DCR between the two groups (P = 0.5917). From the perspective of tumor staging, the DCR of stage III patients (83%) was significantly higher than that of stage IV patients (48%) [Table 5]. The higher DCR was achieved for patients with lung cancer (79%), while pancreatic cancer patients showed the lowest DCR (20%) and was the only group to show a significant difference in DCR when compared with lung cancer patients (P = 0.0161).

Figure 2: The tumor reduction in the typical advanced cancer cases treated with hydrogen inhalation rehabilitation.
Note: (A) Miss Z, 52-year-old, had irritable cough and was diagnosed with positron emission tomography (PET)-computed tomography (CT) scanning in October 27, 2016, showed right middle lung mass (4.1 cm × 3.9 cm) with hilar invasion. (B, C) Bronchial endoscopy showed that a hemorrhagic-erosive lesion was located at the right main bronchus (white arrow), and biopsy showed poorly-differentiated squamous cell carcinoma (C). (D) The patient refused chemotherapy and inhaled hydrogen from November 4, 2016, at least 4 hours a day. After 1 week, the cough was reduced and the breathing became smooth. After 2.5 months, on January 13, 2017, PET-CT was performed and the original lesions in the lungs were not seen. So far, the patient has disease-free survived up to now.

Table 5: Tumor response of stage III and IV advanced cancer patients with hydrogen inhalation rehabilitation
Side-effects of 82 advanced cancer patients treated with hydrogen inhalation rehabilitation
Of the 29 patients treated with hydrogen inhalation alone, no hematological toxicity was found (data not shown for blood routine test), 1 patient developed stomach discomfort and chills, 1 patient developed dizziness (which disappeared spontaneously after several days). Of the 53 patients treated with hydrogen inhalation combination treatments, 1 patient developed headache (which disappeared spontaneously within 3–5 days), 1 developed occasional epistaxis (minor bleeding and gradually resolved), and 1 patient reported dryness of the nasal cavity, which disappeared a few hours after the inhalation stopped.
Discussion
Investigations of the potential of hydrogen to treat tumors have a long history and a great deal of evidence. As early as 1975, Dole et al.[19] reported that hydrogen inhibited cancer. Nude mice with cutaneous squamous cell carcinoma were administered a mixture of 97.5% hydrogen and 2.5% oxygen (at pressure of 8 atmospheres), and the tumor shrank significantly after 2 weeks, while the control group receiving hyperbaric oxygen-helium showed no such changes. In 2008, Saitoh et al.[20] reported that neutral pH hydrogen-enriched electrolytic water inhibited the colony formation efficiency and colony size of human HSC-4 tongue cancer cells while having no significant inhibitory effect on normal tongue epithelioid cells and also inhibited the growth and migration ability of human HT-1080 fibrosarcoma cells. In 2009, Saitoh et al.[21] also reported that enhanced platinum-colloid hydrogen-containing water had an inhibitory effect on the colony formation and size of human HSC-4 tongue cancer cells. In 2011, Zhao et al.[22] found that hydrogen prevented the occurrence of radiation-induced lymphoma. In 2015, Runtuwene et al.[23] reported that hydrogen increased the survival rate of colon 26 carcinoma tumor-bearing mice, induced apoptosis of cancer cells, and enhanced the sensitivity of colon cancer cells to 5-fluorouracil. Our observations of 82 patients with advanced cancers who received hydrogen inhalation therapy with spontaneous breathing suggest that hydrogen therapy acts in four ways. First, hydrogen inhalation therapy improves the quality-of-life of patients. After hydrogen inhalation for 2 weeks, there was significant improvement in breathing, appetite, fatigue and insomnia and after 4 weeks, significant improvements in pain, constipation and diarrhea were observed. Second, hydrogen inhalation therapy can improve physical fitness. After 3 months, lung cancer patients showed the most significant physical improvement, whereas the poorest effect was observed for patients with gynecological and pancreatic cancers. Third, hydrogen inhalation therapy can reduce tumor markers. After 3 months, lung cancer patients showed the most significant reduction in markers, whereas the poorest effect was observed for patients with gynecological, liver and pancreatic cancers. Fourth, hydrogen inhalation therapy can control cancer progression. After 3 months, the tumor control rate of stage III patients was much higher than that of stage IV patients, with the best effect achieved in patients with lung cancer and the worst in those with pancreatic cancer.
The treatment of advanced cancer is a major challenge. Of the cancer drugs approved by the US and European drug administrations, 67% and 57% showed no evidence of long-term survival and improved quality-of-life, respectively.[24],[25] Liang et al.[26] found that the tumor microenvironment associated with chemo- and radiotherapy enhanced the malignancy of cancer cells leading to a stem-like phenotype. In a study of 413 patients with brain metastasis of different causes, Amelot et al.[27] found that anticancer drugs, especially paclitaxel and its derivatives, promoted brain metastasis and reduce disease-free survival of patients. A recent review suggested that all commonly used treatments, including radiotherapy, chemotherapy, fine-needle puncture, and surgery, can cause an increase in circulating tumor cells and promote cancer progression and distant metastasis.[28] Thus, the positive effects of hydrogen inhalation on cancer patients are very encouraging.
According to our follow-up observations, the effect of hydrogen on the control of cancer is not only related to tumor type, but also to the mode of delivery. In this study, hydrogen was inhaled at 66.7%, with a flow rate of 3000 mL/min. Since Ohsawa et al.[29] reported in 2007 that inhaling 2% hydrogen can prevent cerebral ischemia/reperfusion injury, most researchers have used 1–4% hydrogen to study the molecular biological effects of hydrogen. Reports of the effects of high pressure or high concentration hydrogen are rare, although Dole et al.[19] reported that 97.5% hydrogen delivered under 8 atmospheres successfully inhibited skin squamous cell carcinoma. In addition, the extremely high diffusivity of hydrogen provides a guarantee of its rapid delivery throughout the body, as well as a higher requirement for daily and total inhalation time. Yamamoto et al.[30] studied the distribution of hydrogen in rats after continuous inhalation at 3%. The hydrogen concentration in muscle gradually increased with time for the first 20 minutes, reaching the highest concentration in liver and the lowest in kidney. The inhalation time in this study exceeded 3 hours per day, with some patients receiving treatment for 8 hours continuously. It can be speculated that this may account for the fall in tumor markers at 13–45 days (median 23 days) and the appearance of CR and PR at 21–80 days (median 55 days). This is the first report of hydrogen inhalation therapy resulting in decreased tumor markers and tumor shrinkage. Furthermore, in this study, patients inhaled a mixture of hydrogen and oxygen, not pure hydrogen. Hypoxia can induce metabolic modification and promote the progression of malignant tumor adaptively. Conversely, improving hypoxia may inhibit cancer progression.[31],[32] Thus, our findings demonstrate that inhaling oxygen along with hydrogen helps control cancer progression. Finally, hydrogen can be delivered through inhalation, drinking hydrogen-rich water and injecting hydrogen-rich saline. Hydrogen is an inert gas and its solubility in water is very low, so it is difficult to ensure that the required concentration in tissues is achieved by drinking hydrogen-rich water. It has been reported that hydrogen in the brain is undetectable after drinking hydrogen-rich water.[33] Although hydrogen-rich saline injection can rapidly increase the concentration of hydrogen in the blood, continuous infusion of large amounts of saline will cause water-salt retention. Hydrogen inhalation is the simplest method of delivery and inhaling 66.7% hydrogen can achieve rapid rises in hydrogen concentration in tissues, generally reaching a peak of 520 μM within 30 minutes. Sustained hydrogen inhalation maintains high blood levels, equivalent to 600 μM which inhibits cancer cells growth in vitro.[34] The efficiency of hydrogen inhalation is easily affected by the inhalation tool (the efficiency of masks is higher than that of a nasal catheter), the evenness and stability of respiration, and the state of the basic lung function.
In 2014, Hanahan[35] criticized the use of the term “cancer war,” which increased the use of toxic drugs or overly aggressive treatment for incurable cancer. This term resulted in many patients with advanced cancer receiving highly-recommended treatments with severe side-effects rather than being offered access to palliative care. Haines[36] proposed that the time has come to change the term “cancer war.” The selective antioxidant, anti-inflammatory, and signal-conditioning effects of hydrogen may play a major role in improving the cancer microenvironment.[37] More recently, molecular hydrogen has also been associated with immune function, reviving CD8+ T cells in an exhausted state by maintaining mitochondrial function and restoring their anti-tumor function, thus improving the prognosis of patients with advanced cancer.[38] Hydrogen application is simple, with low cost and few adverse reactions, which is an important advantage for patient-centered, family-based home rehabilitation.
This follow-up observation study is the first to show that inhaling high concentrations hydrogen can improve quality-of-life and physical fitness and control cancer progression in patients with advanced cancer. To ensure therapeutic effectiveness, the inhaled hydrogen should be delivered at sufficiently high concentrations to rapid allow entry into tissues, and with enough time to produce a dose-accumulation effect. In this report, we emphasize the importance of rehabilitation and auxiliary intervention, rather than treatment in the general sense. However, more patients of each kind of cancers are required to validate this approach. Further investigations will also clarify issues such as the optimal treatment regimen (dose, duration, mode of delivery and effectiveness of hydrogen rehabilitation combined with mainstream treatment) and the mechanism by which of hydrogen treatment controls cancer (such as removal of reactive oxygen radicals and control of inflammation). This information is important for the development of effective hydrogen therapy for patients with advanced cancer.
Author contributions
Design of the study: KCX, YYL, and XJS; data collection: XFK and FM; data analysis: TYL and SCQ; and manuscript writing: JBC.
Conflicts of interest
There is no conflict of interest.
Financial support
None.
Institutional review board statement
The study protocol received ethical approval from the Ethics Committee of Fuda Cancer Hospital of Jinan University on December 7, 2018 (approval number: Fuda20181207) and conformed to the specifications of the World Medical Association’s Declaration of Helsinki. Written informed consent was obtained from each participant.
Informed consent statement
The authors certify that they have obtained all appropriate patient consent forms. In the form the patients or their legal guardians have given their consent for patients’ images and other clinical information to be reported in the journal. The patients or their legal guardians understand that their names and initials will not be published and due efforts will be made to conceal their identity.
Reporting statement
This study followed the STrengthening the Reporting of OBservational studies in Epidemiology (STROBE) Statement.
Copyright transfer agreement
The Copyright License Agreement has been signed by all authors before publication.
Data sharing statement
Individual participant data that underlie the results reported in this article, after deidentification (text, tables, figures, and appendices). Study protocol and informed consent form will be available immediately following publication, without end date. Results will be disseminated through presentations at scientific meetings and/or by publication in a peer-reviewed journal. Anonymized trial data will be available indefinitely at www.figshare.com.
Plagiarism check
Checked twice by iThenticate.
Peer review
Externally peer reviewed.
Open access statement
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical






